
From the 1Evidence-based Insurance Medicine (EbIM) Research and Education, Department of Clinical Research, University of Basel Hospital, Basel, Switzerland, 2Amsterdam University Medical Center, Location Academic Medical Center (AMC), Coronel Institute of Occupational Health, APH Institute, Amsterdam, The Netherlands, 3Research Center for Insurance Medicine (KCVG), Amsterdam, Netherlands, 4German Pension Insurance, Department Social Medicine and Rehabilitation, Berlin, Germany, 5Division of Insurance Medicine, Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden, 6Swiss Insurance Medicine, c/o Medworld, Steinhausen, Switzerland, 7National Alliance of Christian Mutualities, Department of Medical Management, Brussels, Belgium, 8Council of Choices in Health Care, Ministry of Social Affairs and Health, Helsinki, Finland, 9National Health Insurance Fonds, Paris, France, 10Healthy Working Lives Group, Institute of Health and Wellbeing, College of Medical, Veterinary and Life Sciences, University of Glasgow, United Kingdom, 11Achmea, Tilburg, The Netherlands, 12European Union of Medicine in Assurance and Social Security, Brussels, Belgium and 13Amsterdam University Medical Center, Location VU University Medical Center, Department of Public and Occupational Health, APH Institute, Amsterdam, The Netherlands
Objective: To perform a European survey of the evidence needs and training demands of insurance medicine professionals related to professional tasks and evidence-based practice.
Design: International survey.
Subjects: Professionals working in insurance medicine. Methods: Experts designed an online questionnaire including 26 questions related to 4 themes: evidence needs; training demands; evidence-seeking behaviour; and attitudes towards evidence-based medicine. Descriptive statistics were presented by country/conference and the total sample.
Results: A total of 782 participants responded. Three- quarter of participants experienced evidence needs at least once a week, related to mental disorders (79%), musculoskeletal disorders (67%) and occupational health (65%). Guidelines (76%) and systematic reviews (60%) were the preferred types of evidence and were requested for assessment of work capacity (64%) and prognosis of return- to-work (51%). Evidence-based medicine was thought to facilitate decision-making in insurance medicine (95%). Fifty-two percent of participants felt comfortable finding, reading, interpreting, and applying evidence. Countries expressed similar needs for reviews on typical topics.
Conclusion: This study reveals evidence gaps in key areas of insurance medicine, supporting the need for further research, guidelines and training in evidence-based insurance medicine. Importantly, insurance medicine professionals should recognize that evidence-based practice is crucial in producing high-quality assessments.
Key words: social security; disability evaluation; return to work; evidence-based practice; quality assurance; surveys and questionnaires; guidelines.
Accepted Mar 11, 2021; Epub ahead of print Mar 29, 2021
J Rehabil Med 2021; 53: jrm00179
Correspondence address: Regina Kunz, Evidence-based Insurance Medicine (EbIM) Research & Education, Research and Education, Department of Clinical Research, University of Basel Hospital and University of Basel, Spitalstrasse 8+12, 4031 Basel. E-mail: regina.kunz@usb.ch
Doi: doi: 10.2340/16501977-2821
Evidence-based medicine (EBM) means the consideration of research findings when taking decisions in clinical medicine. This approach has become standard in health and social care. Since it is less clear to what degree EBM is applied in insurance medicine, European insurance physicians performed a joint survey among colleagues in 8 countries and 2 conferences. More than 700 professionals participated. Half of respondents experienced a need at least once a week to look for guidelines and systematic reviews about work capacity assessments related to mental or musculoskeletal disorders. Almost all thought that EBM would facilitate decision-making. Not all felt competent in finding, reading, interpreting, and applying research evidence. Overall, findings were similar across countries. These results illustrate important evidence gaps in insurance medicine, supporting the need for further research and guidelines. Importantly, professionals should recognize that evidence-based practice is crucial in producing high-quality assessments.
Medical experts in insurance medicine (IM) conduct assessments on health-related issues for public and private insurance schemes (e.g. disability pension, sickness allowance, life and health insurance, and compensation following accidents). Common tasks of IM experts include work disability evaluation, promotion of return-to-work and societal participation of individuals with disabilities, assessment of impairments and causality, sick-leave certification, risk assessments for private insurers, and monitoring and analysis of healthcare consumption (1). This task-based definition of IM offers strong cohesion across countries, settings, legal frameworks and constituencies.
While the medical core tasks in IM are similar across countries (1), their organization varies. Some countries, such as the Netherlands, regard insurance medicine as a distinct medical discipline with its own canon of knowledge, skills and experience, and a board examination after 4 years of training, while other countries are satisfied with the skills set that medical professionals acquire during medical training and enhance in specific courses as needed (e.g. Germany, Switzerland, Sweden). All countries, however, agree that practising doctors and IM professionals need specific knowledge and skills in IM.
Furthermore, IM is always embedded in a legal framework of social policy (2), which is likely to impact on the way research evidence will be used in different settings. This feature, however, is not unique to IM; it rather applies to the production and implementation of health services research in general, at the local, regional, national and international level (3, 4).
Judgements and recommendations provided by medical experts have significant implications on the reliability of medical assessments (5), the fair, equitable and efficient allocation of resources (6) and, ultimately, the financial sustainability of social security systems. A recent systematic review about the level of agreement among experts evaluating work disability found only low-to-moderate reproducibility in their judgements of work capacity and highlighted the need for research to improve the quality of disability assessments (7). In recent years, most industrialized countries experienced a substantial increment in disability benefit payments (8). A shortage of experts with competences for supporting return-to-work in sick-listed individuals was considered a key barrier to counteract this trend (9).
Insurance schemes (e.g. disability vs accident vs healthcare insurance) differ in the kind of medical evidence they need to inform their specific tasks. Anecdotes indicate that the body of evidence with relevance to these specific tasks is sparse (10). Medline, the most comprehensive medical database, with more than 32 million records from more than 5,500 journals (“Pubmed all[sb]” National Library of Medicine Systems, Bethesda, USA, retrieved 2021 Feb 6) has more than 45 insurance-related search terms (so-called “Medical Subject Headings”) that allow systematic retrieval of relevant studies. The vast majority is related to economic, organizational, technical, and administrative issues of healthcare. However, the term “insurance medicine” is missing. Consequently, experts tend to rely on expert opinions, personal experience, and common sense when providing recommendations. Clinical medicine has replaced the eminence approach as the basis for action with an explicit evidence-based medicine (EBM) approach, and this evolvement is slowly changing IM too (11, 12). Searching, compiling and accessing IM evidence is, however, challenging. The lack of international scientific journals dedicated primarily to IM means that authors publish IM research in any journals with a clinical focus. This scattering of IM evidence is a major obstacle to the efficient dissemination of IM research. Furthermore, levels of professionalization vary substantially among countries. Training opportunities for developing EBM-skills with a focus on the specific needs of IM beyond interventions (i.e. research on prognosis or causality) are missing.
The aims of this study were to identify and illustrate the evidence needs and training demands of European insurance physicians and other healthcare professionals related to professional tasks and evidence-based practice in IM, irrespective of the countries’ approaches to organizing the provision of IM and the legal frameworks embedding it.
Study design
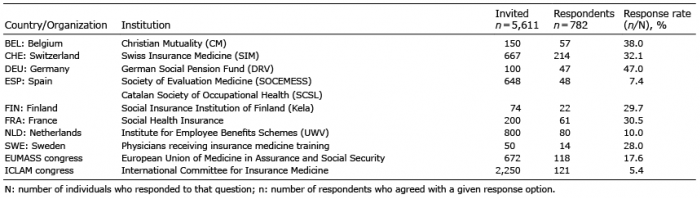
An online survey was performed in 8 European countries and among attendants of the international conferences of 2 IM associations, the European Union of Medicine in Assurance and Social Security (EUMASS) targeting social insurance physicians and the International Committee for Insurance Medicine (ICLAM) targeting private insurance physicians (Table I and Appendix S1). The survey was in agreement with the principles of the Declaration of Helsinki (13): the introduction to the survey informed participants about scope, confidentiality policy (collection of anonymous data and their reporting as aggregate data), and their consent to the study by submitting the survey. In-house funding, the lack of conflict of interest of authors, and the potential conflict of interest of R. Kunz due to her part-time employment with the Swiss National Accident Insurance Funds, were reported in the paper. Given the absence of sensitive data (14) in the survey, no formal ethics vote was obtained. To guide the reporting of introduction, methods, results, and discussion, this study followed, as applicable, the recommendations for reporting survey research by Bennett (15), which were based on critical analyses of 4 checklists on the conduct or report of survey research and an empirical analysis of guidance to authors from 20 top medical and specialty journals.
Table I. Response rates by country or organization. See Appendix S11 for details of the institutions
Description of the questionnaire
The questionnaire was a self-administered instrument developed by 6 IM experts (W. de Boer, E. Friberg, J. Hoving, R. Kunz, F. Schaafsma, R.Weida-Cuignet) from the Netherlands, Sweden and Switzerland. It encompassed 26 items addressing 5 domains: characteristics of respondents (3 items), area of work and work experience (4 items), information needs and training demands (5 items), information-seeking behaviour (4 items), and attitudes towards, knowledge and skills in EBM and Cochrane (10 items). The construction of the questions followed the guidance by Woodward et al. (16). Questions were closed-ended, semi-open or free text, with single or multiple choices or Likert scales. Based on the piloting among 34 Dutch insurance physicians and the input from the experts, the wording of some questions was modified slightly, omitting 2 questions as referring too much to the Swiss system, and the sequence of the questions within the survey was re-arranged. The survey was finalized in English and translated into German, French and Spanish. Completion of the survey took 10–15 min. The verbatim questions and participants’ responses are reported in Appendices S2–S61.
Administration of the questionnaire
The survey targeted a heterogeneous spectrum of insurance physicians employed by disability, accident or health insurers (in Belgium, Finland, France, Germany, Netherlands, Spain and Switzerland), medical practitioners performing tasks for insurers, such as sick-leave certification (Sweden, Switzerland), and other health professionals, researchers and managers (Switzerland, Belgium), including attendants of the EUMASS and ICLAM conference 2016. Countries used various sampling methods. Contacts within national IM organizations recruited IM professionals by sending out invitations to complete the survey linked to the on-line survey platform SurveyGizmo (Gizmo transformed to Alchemer in Oct 2020 available from: https://www.alchemer.com/). Participation was anonymous. The survey used an adaptive design, allowing respondents to skip questions, to modify their answers prior to submission and to withdraw at any time. The survey did not enforce answers. Data collection took place between February and October 2016. In general, the first invite was followed by 2 reminders. One group circulated 1 reminder only, 2 groups circulated 3. The survey did not use incentives to encourage participation. The first page of the survey provided information on scope, confidentiality policy and that participation indicated agreement with the policy. Survey data were anonymous and did not contain sensitive data.
Data analysis
All questionnaires with at least one question beyond the sociodemographic variables completed (i.e. complete and partially complete questionnaires) were included. Since answers by participants were not enforced, the number of respondents could vary by question. Agreement with a response option was therefore reported as the ratio of the number of respondents who agreed with any given response option (numerator, expressed as ‘n’) to the total number of individuals who responded to that question (denominator, expressed as ‘N’). Answers were dichotomized on a Likert scale (e.g. pooling “very comfortable” and “somewhat comfortable” as “comfortable”), where appropriate. Absolute and relative frequencies were calculated and descriptive analyses of continuous and categorical variables were performed. Response rates represent the number of returned questionnaires divided by the number of questionnaires sent out, and were reported by country or population level. The sampling method did not allow analysis of undelivered or received e-mails, or non-responders and their characteristics. The findings were compared visually. The variation between conferences and nation-al organizations were considered as a difference if the results of the conference were outside the range of the 8 countries. For instance, S4-Q4.3: On what kind of topics would you need evidence the most? Answer option: Prognosis of disease. Agreement with the answer option by country ranged from 51% (Netherlands) to 17% (France). In contrast, 62% of the attendents of the ICLAM conference voted for this option. Conferences for social and private insurance physicians were examined separately to take into account their different tasks (e.g. disability assessment vs risk assessment) related to the focus of their organizations. Descriptive statistical analyses were carried out using SPSS 22.0 for Windows (IBM, Armonk, NY, USA).
Characteristics of respondents
From 5,611 invitations circulated through our professional network, 782 professionals from 8 national organizations (almost exclusively linked to social insurance) and 2 international IM conferences (EUMASS and ICLAM) returned the survey (Table I and Appendix S1), with 693 respondents providing data beyond socio-demographic information. The overall response rate was 30% (median), ranging from 47% (Germany) to 5% (ICLAM). Results per country and conference are reported in the Appendices.
The mean age of respondents was 53 years (range 25–82 years), 47% were female (n = 660). Ninety-seven percent worked in Europe, the majority (72%; n = 661) felt comfortable using English as working language.
Areas of work and work experience (Appendix S2)
Participants were experienced IM professionals, with a mean work experience of 21 years (range 1–58 years). They worked as practitioners with or without patient contact (48% and 19%, respectively), healthcare professionals (36%), managers (19%), educators (11%), researchers (10%), or staff members (7%) (n = 743). Their main tasks were evaluating work disability (82%), promoting return-to-work (57%), certifying sick-leave (41%), assessing risks (27%), and monitoring and governing the provision of healthcare (23%) (n = 730).
Evidence needs
Respondents reported looking for evidence on a daily, weekly, or monthly basis (31%, 42%, 20%, respectively; n = 693). Mental disorders, musculoskeletal disorders, and work-related health complaints (79%, 67%, 65%, respectively; n = 646) were named as medical fields with high priority for more evidence syntheses (Table II). Respondents reported evidence needs for their IM tasks (Table III), e.g. when assessing work capacity, making prognostic predictions on return- to-work, or verifying the presence of subjective health complaints (64%, 51%, 51%, respectively; n = 660).
Evidence-seeking behaviour (Appendices S3 and S4)
To cover their evidence needs, professionals accessed scientific journals, approached colleagues, used textbooks and attended scientific conferences (79%, 66%, 50%, 44%, respectively; n = 674). They preferred guidelines and systematic reviews, followed by case law, and primary studies (79%, 60%, 40%, 33%, respectively; n = 645). Systematic reviews (89%; n = 376), guidelines (80%; n = 487), scientific journals (80%; n = 496) and scientific conferences (71%; n = 281) were considered as the most updated and most accurate sources of evidence. Sixteen percent of respondents (n = 695) lacked, or were unaware of, access to scientific evidence through databases such as PubMed or Embase.
Table II. Priorities for health topics in need of more evidence (n = 646). The question was: “From which medical field do you need evidence most urgently? (Multiple options)
Table III. With reference to the core tasks of physicians in insurance medicine and social security (1), evidence on what topics would you need the most? (Maximum of 3 options; n = 660)
Evidence-based medicine and Cochrane: attitudes, knowledge, and skills (Appendices S4 and S5)
Almost all respondents considered EBM as a method to enhance decision-making in IM (95%; n = 686). Half of the respondents had participated in at least 1 course on EBM over the past 10 years (50%; n = 663). Overall, when asked about their skills in finding evidence (n = 682), 51% of respondents felt comfortable, while 45% would welcome training. With regards to readings skills (n = 674), 63% felt comfortable, while 36% would welcome training. With regards to the skills in interpreting studies (n = 668), 44% felt comfortable, while 52% would welcome training. With regards to skills in applying evidence to cases (n = 656), 48% felt comfortable, while 47% would welcome training (Table IV).
Forty percent of participants had never heard of Cochrane or their goals and activities (40%; n = 662), while 7% had at some point been involved with the Cochrane Collaboration. One-third confirmed access to the Cochrane Library at their workplace (36%; n = 556), whereas 30% were uncertain. Half of participants had searched the Cochrane Library at least once (50%; N=554). From those who had run a search in the past 4 weeks, 25% (n = 256) found the information they were looking for, and 90% (n = 64) considered the retrieved evidence helpful. When asked about their skills in reading, the majority of participants found the abstract and plain language summary of a Cochrane review easy to understand (both 70%; n = 434), and just over half of the participants considered the entire article easy to understand (55%; n = 433).
Contrasts across countries and conferences
Only a few differences emerged across national organizations and between organizations and attendants of conferences for private and social insurance (Appendices S2–S6). Observed differences were better explained by context and related tasks of social or private insurance physicians (Table II and III) than by setting (i.e. national organization vs conference). The perceived need for more evidence syntheses across countries and IM associations showed a rather homogenous pattern for almost all questions. Private insurers and Dutch respondents deviated somewhat from the general coverage by expressing higher evidence needs for cancer and cardiovascular disease and for the assessment of health-related risks for life insurance (private insurers).
Table IV. Perceived competences and training demands in the techniques of evidence-based medicine
Summary of the findings
This first European survey on EBM in IM documents the needs and expectations of European IM physicians and related professionals. In this survey, respondents experienced a lack of evidence syntheses in key medical areas, i.e. mental and musculoskeletal disorders, work-related health complaints related to IM tasks, such as work capacity assessment, prognostic predictions, and verification of subjective conditions. They considered systematic reviews and guidelines as trustworthy and up-to-date sources of evidence and EBM as a key method to enhance the quality of IM practice. The findings were consistent across countries, social security systems, and IM associations. Half of the respondents felt competent with the methodology of EBM, while the other half welcomed training.
Attitudes of other insurance medicine professionals
A decade ago, a survey exploring the attitudes of
Belgian insurance physicians towards EBM and clinical practice guidelines showed very positive attitudes, but also revealed a lack of specific knowledge and skills in practice (11). Lack of time, of EBM skills, and of needed evidence were reported as the most important barriers. The authors disagreed that differences in social legislation across countries may act as barrier to EBM, since all regulations expect “insurance physicians … to be able to correctly assess each medical condition based on good evidence”. Authors envisioned evidence-based clinical guidelines and global access to this information to be a way of making evidence directly applicable; a view that was shared by others (11, 17, 18).
A more recent survey in the workers’ compensation setting investigated the attitudes of Australian health professionals towards using electronic EBM guidance by an US company for decision-making (19–21).
Positive feedback referred to specific recommendations on issues such as treatment intensity (e.g. “evidence-based” numbers of physiotherapy sessions), expensive diagnostics (e.g. magnetic resonance imaging (MRI) scans) to limit over-servicing, and guidance to manage expectations by claimants (e.g. timely return-to-work) or claims managers (e.g. the medically required duration of recuperation). Concerns addressed that rigid applications of the evidence tool may result in unfair denials, inappropriately standardized treatment of
claimants (22) or ignoring cultural differences in values and preferences (22).
Insurance medicine and guidelines
As observed in this survey, clinical practice guidelines have become an important and trusted reference to advise IM practice. Various social security systems and professional organizations have started to develop evidence-based IM guidelines, with a methodological framework, focused questions and a comprehensive background document. For instance, the recently updat-ed Dutch “Guideline on low back pain and lumbosacral radicular syndrome for occupational and insurance physicians” (23) consists of a 2-page summary card, a 23-page short version of the guideline and a 223-page background document with the evidence underpinning the recommendations (24). The guideline developers used a transparent approach to grade the certainty (previously “quality”’) of the evidence and the strength of the recommendations known as Grading of Recommendations Assessment, Development and Evaluation (GRADE). This example illustrates that available evidence, albeit limited, allows to develop guidance, albeit sometimes preliminary, while identify-ing critical evidence gaps for further research.
Guidelines can improve quality. Following the introduction of national evidence-based guidelines on sickness certification, more than 80% of Swedish primary care physicians valued the guidelines as benefi-cial to the patient encounter and to ensure quality in sickness certification (25). However, even 4 years later, a
quarter of these physicians still identified a need for more knowledge and competences regarding IM.
Producing evidence-based guidelines requires a sizeable amount of work and resources. Avoiding duplication of efforts would be highly desirable. Sharing international evidence, while providing recommendations in line with local circumstances and legal context, has been a longstanding vision of EBM (3). To that end, in 1995, when Canadian insurers were confronted with increasing claims for whiplash-associated disorders (WAD) caused by car accidents and a lack of effective strategies to deal with them, the Quebec Task Force on Whiplash was established (26). The Task Force’ exhaustive compilation of evidence formed the foundation for organizational, local, national and international recommendations on WAD management for treating and insurance physicians alike and stimulated research on evidence gaps (27). Two other “Best Evidence Syntheses” by the WHO on Mild Traumatic Brain Injury (MTBI) (28, 29) and MTBI prognosis (30), conditions with unspecific symptoms and unclear prognosis commonly faced by accident insurers, had similar impact. Expanding this idea of sharing the work-up of the evidence and testing it with other common and costly conditions would be a worthwhile undertaking.
Insurance medicine and systematic reviews
In the current survey, only one-third of the total respondents who had recently searched the Cochrane Library (for many an indicator for evidence-based practice), reported having found the evidence they had sought. Both figures may raise concerns about the searching skills of IM practitioners, the retrieval rate of suitable Cochrane reviews, or the extent to which Cochrane reviews actually cover topics of relevance to IM.
Searching the Cochrane Library and other resources of IM evidence can be a challenge. IM evidence is often best identified by outcome, such as work disability, return-to-work, time off-work, participation, or cost. Most trials and reviews, however, report these endpoints as secondary outcomes only (e.g. return-to-work in a drug trial on multiple sclerosis) or as surrogate outcomes indirect to the clinically relevant outcome (e.g. duration of hospital stay indirect to return-
to-work) (31). To overcome this barrier, the Cochrane field “Insurance Medicine” (32) recently created the topic “Insurance Medicine” in the Cochrane Library with the aim of improving retrieval of relevant reviews (33) (www.cochranelibrary.com/browse-by-topic). To date, more than 420 Cochrane reviews and more than 220 protocols have been tagged with the searchable
topic “Insurance Medicine” (last accessed 2021 Feb 12).
Cochrane, with its focus on healthcare interventions, has very limited coverage of systematic reviews on causality or on prognosis, research findings that IM professionals need for medical assessments. Existing research on IM topics needs to be compiled and made available in other ways. We envision a specific database for medical research in the context of social security and insurance medicine. A first pilot is “Evidence on the web” (https: //insuremed.cochrane.org/evidence), showcasing bibliographies of systematic reviews on a variety of topics and related to IM tasks (1), published in the Cochrane Library and the general medical literature. To cover their need for evidence, IM professionals require access to both kinds of collections; Cochrane reviews and non-Cochrane evidence.
Strengths and limitations
An international group of researchers developed and disseminated the survey across 8 countries to a diverse spectrum of IM professionals, and to interdisciplin-ary IM organizations and conferences. Dissemination mainly in national languages reduced barriers to participation (34). The survey therefore captures Europe’s heterogeneous landscape in social security. Consistent findings across countries challenge the common belief that evidence needs are mainly
country- or legislation-specific (3, 11), and strengthen the notion that IM encounters similar challenges across Europe (10). Reported evidence needs related mainly to disability, whereas tasks related to accidents, such as verifying causality, or to private insurance, such as risk assessment ranked lower. This observation may reflect the higher number of disability claims due to health impairments compared with accident claims in society, and therefore the number of physicians working in each area.
To better understand inconsistent findings, such as self-reported high level EBM-skills vs lack of familiarity with Cochrane, may require qualitative approaches, such as free-text sections in the survey, or add-on interviews among subgroups. Sending out varying rounds of reminders in our survey (1–3 rounds, with a mean of 2) might have led to response bias by missing individuals who did not respond to the initial invite plus first reminder, but would have responded to follow-up reminders. Empirical evidence, however, identified the initial invite as key, with low return (35) and lower data quality (36) in reminders, but no additional recruitment of actual “non-responders” with different features compared with respondents from the first invite (37). One might argue that the moderate response rate (compared with earlier surveys on the topic (11, 12)), missing information about non-respondents, and the respondents’ high comfort level with EBM suggest the presence of participation bias (11), where those with experience in EBM were more likely to participate. This cautions generalizations of the results to the IM community as a whole. On the other hand, the views of professionals knowledgeable in both areas, IM and EBM, can serve as expert guidance on how to advance the practice of EBM within IM.
Terminology varies across countries. While some countries call the discipline “Insurance Medicine”, other participating countries attribute the same activities to “Social Security” or consider it an activity of social medicine. Heterogeneous terminology for the same kind of work can also be found in other areas of medicine. For instance, the terms “family physician”, “primary care physician”, “’general practitioner”, “general physician”’, “general internist”’, or “medical generalist” reflect similar, but not identical, professional activities. Such heterogeneity is not a problem as long as similarities and differences are explained if required. In the current study, we used the terms “Insurance Medicine” and “Social Security” interchangeably.
Implications for knowledge translation
Based on the survey results, communication with the IM community in Europe and various knowledge translation frameworks (38–40), we developed recommendations for knowledge translation strategies that focus on evidence production, dissemination, access, use, and advocacy (Table V). With regards to production, the current study identified evidence needs in broad medical areas and IM tasks. These areas need to be refined into priority research questions for the production of primary studies, systematic reviews and guidelines. Dissemination strategies should include scientific journals, Cochrane Insurance Medicine, professional organizations, academic events and congresses. Language barriers were identified and the need for translating evidence into other languages besides English. Future research should explore user preferences of novel formats for summarizing (e.g. podcasts, Cochrane corners, blogs, videos) and disseminating evidence (e.g. social media, Wikipedia). To improve access, efforts should address the viability of an IM database for systematic reviews and primary studies and thus facilitate evidence-based practice in IM. To increase the use of evidence in practice, programmes teaching competences and skills to insurance physicians,
decision- and policymakers, will be required. Advocacy
efforts need to identify priority research questions and increase funding and production of primary and secondary research. Implementation strategies need to improve the compilation of and access to evidence. Table V provides a summary of our recommendations.
Table V. Knowledge translation strategies to get insurance medicine evidence into practice
Conclusion
In conclusion, the current survey shows that EBM has not yet become standard in IM practice, despite ap-proval by the vast majority of IM professionals. Reasons such as unfamiliarity, difficulty with searching and using evidence or a shortage of IM-related evidence account for the deficit. All these reasons warrant endeavours in generating evidence and transferring it to those in need. However, above all, IM professionals should recognize that evidence-based practice is crucial in producing high-quality assessments and recommendations.
Nomenclature
This paper uses the terms “insurance medicine” and “social security” interchangeably, mainly with reference to work disability and accident insurance. Insurance medicine/social security refers equally to healthcare and other types of health-related insurance.
The authors thank Brigitte Walter Meyer and Sacha Röschard for their support in administrative and data management tasks, and the many insurers, organizations, conference organizers who supported the survey by circulating it to their members, conference delegates, stakeholders, and constituents.
Conflicts of interest. Conflict of interest disclosure forms were collected from all contributors. ReKu declared a part-time employment with the Swiss National Accident Insurance Funds, a national not-for-profit organization with a public mandate. All other authors had no conflicts of interest to declare.
Funding. The survey was not funded by external sources.


 Click to show fullsize
Click to show fullsize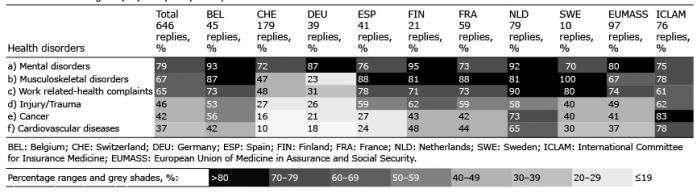 Click to show fullsize
Click to show fullsize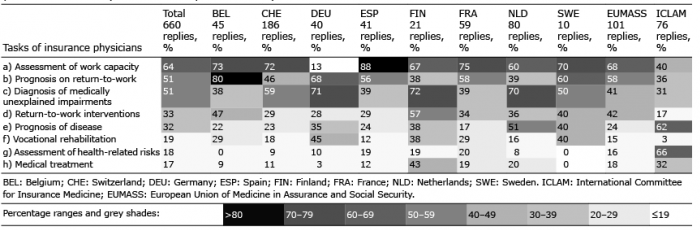 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize